
What does this mean? Should you still seek treatment for a disc herniation or just wait for it to go away on its own?
“The existing evidence shows that the overall resorption incidence of lumbar disc herniation (LDH) was 70.39%, the resorption incidence of ruptured LDH is higher than that of contained LDH.” (Zou et al.)
“The probabilities of spontaneous regression (were):
- Bulging 13.3%
- Protruded 52.5%
- Extruded 70.4%
- Sequestered 93.9%
Extruded and sequestered discs were also significantly more likely to completely regress than smaller morphologies.” (Rashed et al.)
What does this mean?
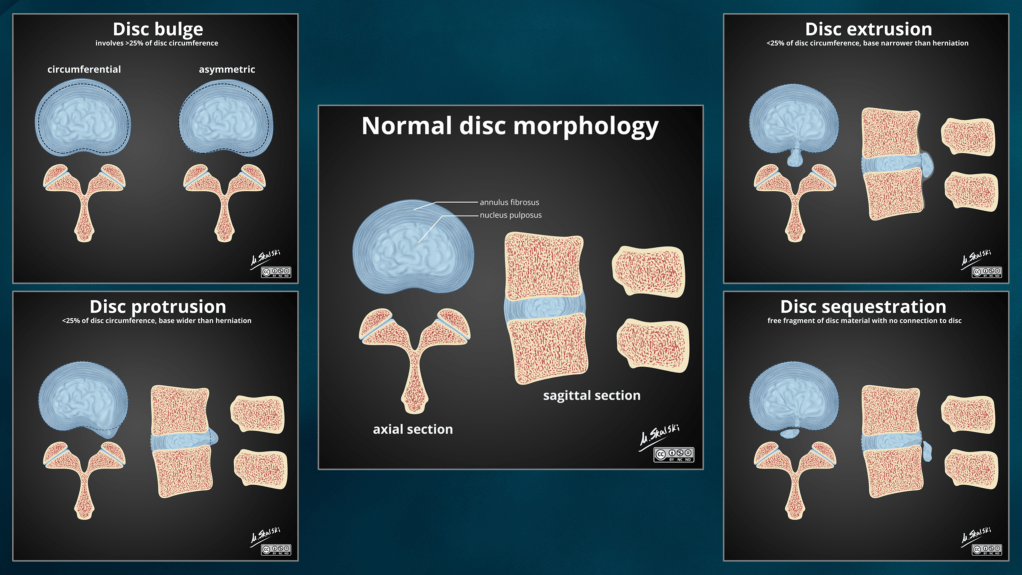
A disc herniation happens when the soft cushion-like disc between your vertebrae bulges or ruptures. Think of it like a jelly-filled donut: the jelly (the disc nucleus) pushes out through a tear in the outer dough layers (fibrous disc wall called the annulus), it can press on nearby nerves, causing pain, numbness, or weakness in an arm or leg.
There are 4 types of disc herniations as listed above. A bulging disc is when some of the annulus fibers stretch or become slackened extending a portion of the disc (more than 25% of the circumference) beyond the border of the neighboring vertebrae. A protrusion and extrusion are similar, but are defined by their measurements. A protrusion is wider at its base than it extends away from the normal disc space. An extrusion is narrower at it’s base and extends further away from the normal disc space. A sequestration is a special subclassification of disc herniations where the nuclear material not only pushes out of the normal disc space but it detaches from the rest of the disc.
As evidenced by the findings in the two studies cited above, our body often recognizes that there is an issue with the herniated disc and mounts a response in an effort to return the disc to as normal a state as possible. The more disc nucleus that is ruptured through the annulus the greater a response we see mounted by the body.
So does that mean I should just wait for the herniation to go away?
Not necessarily. Depending on the severity of the symptoms you are experiencing you may experience lasting repercussions from not seeking treatment. Or you may simply not want to deal with the lingering pain, numbness, or tingling that can be seen in patients with disc herniations.
If I have a herniation do I need surgery?
Maybe. But many people find tremendous relief of their symptoms from conservative care such as chiropractic and physical therapy. In fact, many insurance companies require you to undergo a trial of conservative care before they will approve you as a candidate for surgery.
Also, studies have shown there is not always a correlation between imaging findings and symptoms experienced by patients. Meaning just because your doctor tells you there is a herniation, or another abnormality, on your X-ray or MRI does not mean you will experience any symptoms from it. Conversely, you may be experiencing symptoms but find that there is frustratingly little to see on any imaging reports.
Can a chiropractor help?
Absolutely! As mentioned above conservative care is often the place to begin for your disc herniation, and chiropractic is a great choice for that care. Your chiropractor can use a combination of pain relief modalities (electric stim, cold laser, etc.), flexion distraction, spinal manipulation/mobilization, exercises, or other noninvasive techniques to help alleviate your symptoms.
What does surgery for a herniation look like?
If it is determined that you do need surgery for your disc herniation there are a couple different options that your surgeon may consider. They may go in and remove the portion of the disc that is herniated. Alternatively, you may have a procedure known as a laminectomy that removes a portion of the vertebra in an attempt to relieve pressure on any nerves in the area. Your surgeon may also recommend a spinal fusion surgery where the vertebrae above and below the disc are fused together. However, this alters the biomechanics of your spine and can cause other complications down the road. A newer procedure called Artificial disc surgery (ADS) is an alternative to spinal fusion. In ADS, the surgeon replaces your damaged disc with an artificial one.
Each of these procedures have their own risks associated with them and recovery times. There also is the consideration that once an individual has an initial surgery to their spine their odds of needing surgery in the future rises dramatically. Surgery should never be entered into lightly, but especially spinal surgery.
Note: There are times where surgery is a more immediate consideration. Symptoms such as a loss of sensation within the "saddle" area of your legs and pelvis, or new difficulties with bowel/bladder function may indicate to your doctor that you could need surgery now.
If you have questions, would like more info, or would like to schedule an appointment please feel free to reach out to our office!
Zou T, Liu XY, Wang PC, Chen H, Wu PG, Feng XM, Sun HH. Incidence of spontaneous resorption of lumbar disc herniation: a meta-analysis. Clinical Spine Surgery. 2023 Jul 31:10-97. Link
Rashed S, Vassiliou A, Starup-Hansen J, Tsang K. Systematic review and meta-analysis of predictive factors for spontaneous regression in lumbar disc herniation. Journal of Neurosurgery: Spine. 2023 Jul 14;1(aop):1-8. Link
